
Research article/ Open Access
DOI:10.31488/EJRM.157
Risk Factors of Active Tuberculosis and Tuberculosis Outcomes in Patients with Diabetes Mellitus: A Retrospective Matched Case-Control Study
Trirong Choosongdet M.D.*1, Gompol Suwanpimolkul M.D.2,5, Thanawat Nochaiwong3 , Jiratchaya Sophonphan3, Anchalee Avihingsanon M.D.3,5, Kamon Kawkitinarong M.D.4,5
1. Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
2. Division of Infectious disease, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
3. HIV Netherlands Australia Thailand Research Collaboration, the Thai Red Cross AIDS Research Centre, Bangkok, Thailan
4. Division of Pulmonary and Critical Care Medicine, Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
5. Centre of Excellence in Tuberculosis, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
*Corresponding author: :Dr. Trirong Choosongdet, M.D, Respiratory and Critical Care Physician Division of Respiratory and Critical Care Medicine Department of Internal Medicine Surin Hospital, Thailand, Email: memorizer.dx@gmail.com
Abstract
Diabetes mellitus (DM) increases the risk of mortality and morbidities related to active tuberculosis (TB). Both diseases are common interlinked, particularly in high TB prevalence countries. Identifying the specific characteristics of patients with DM who later develop tuberculosis disease is crucial in promptly screening and early diagnosis of active TB. We therefore aimed to assess the predictor of active TB and TB treatment outcome among DM participants in Thailand. We conducted a retrospective cohort of 764 diabetic patients from January 2015 to December 2019 at King Chulalongkorn Memorial Hospital. Patients were categorized into “TB” and “no TB” group. To determine factors associated with incident TB were analyzed using Cox proportional hazard regression was done with 95% CI and p value < 0.05 considered significant. Out of total 764 diabetic patients, there were 509 DM without TB, 255 DM with TB. Of 255 DM with TB. 57 participants had DM at time of TB diagnosis. Overall prevalence of HIV infection was 2% and median age was 62.8 (QR 53.6-72.5) years. Median year of follow-up was 3916.2 person-years follow-up, the TB incident rate among diabetic patients was 45.96 (95%CI 39.72-53.19) per 100 person-years follow-up. The median HbA1c at the TB diagnosis was 8 (IQR 6.6-10.3). In multivariate analysis BMI<18.5 (aHR 3.78; 95%CI 2.47-5.78; p<0.001), smoking (aHR 1.95; 95%CI 1.23-3.10; p=0.004), HIV infection (aHR 3.31; 95%CI 1.59-6.86; p=0.001) were associated with active TB. Additionally, type of DM treatment was also related to active TB; insulin injection (aHR 1.60; 95%CI 1.02-2.51; p=0.04), combination treatment (aHR 1.66; 95%CI 1.02-2.70; p=0.04) and diet control (aHR 2.50; 95%CI 1.24-5.04; p=0.01) when compared with oral hypoglycemic drugs. Among TB cases, TB cure or treatment completion was 71.8%; 6.7% had TB relapse and 13.7% had drug resistance. Mortality rate of TB cases was 12.9%. The incidence of TB among DM cases observed in this study was high and it was associated with low BMI <18.5, smoking and HIV infection, pointing to the need to pay attention to these factors when managing this co-morbidity
Introduction
Tuberculosis (TB) is a common infectious disease in Thailand. Thailand is listed of one of the 14 countries with high tuberculosis burden in the world. It is estimated that the annual number of new cases is approximately 120,000 with 12,000 deaths, and 2,200 cases of multidrug-resistant tuberculosis per year were reported. The National Tuberculosis Prevalence Survey in 2012- 2013 estimated that the incidence rate of TB in 2014 was as high as 171 per 100,000 population [1].
Thailand has a newly diagnosed TB rate of 1.3 times which is higher than the global average, but only 59% of the estimated cases detected and reported. This reflects delayed or inaccessible treatment for some patients, causing the spread of this infection to the community. and decrease the morbidity rate. Consequently, Thailand needs a strategy to halt the TB sequelae such as a high emerging rate of new infection and MDR TB infection [1].
Tuberculosis (TB) is a contagious disease caused by Mycobacterium tuberculosis. Tuberculosis can infect any organ of the body, especially in the lungs (80%), where it can be easily transmitted. Extrapulmonary tuberculosis may be found in other organs such as pleura, lymph nodes, spine, peritoneum, etc. Only about 10% of latent tuberculosis have symptomatic TB [2]. The likelihood of developing the disease increases in patients with low immunity, such as HIV infection and diabetes. Screening for those patients is important to early diagnose tuberculosis, reduce the spread of infection and have better treatment results. There are many studies on the risk of HIV co-infected with tuberculosis. However, the data on patients with diabetes remain lacking.
Several high-quality cohort studies have shown that diabetes is at an increased risk of developing active tuberculosis compared to general population and that those with poor diabetic control may be vulnerable [1,3-6]. The cause of the elevated risk is unclear and has not been thoroughly investigated.
Methods
Study population
This retrospective matched case-control study was carried out in diabetic patients treated at outpatient department of King Chulalongkorn Memorial hospital from January 2015 to December 2019 and we excluded the incomplete data patient from this study
Selection of case and control
The case group consisted of tuberculosis in diabetics. The control group consisted of diabetes patients who do not have tuberculosis in the King Chulalongkorn Memorial hospital database from January 2015 to December 2019. Regarding the number of controls per case, a 2:1 ratio was adopted.
Statistical analysis
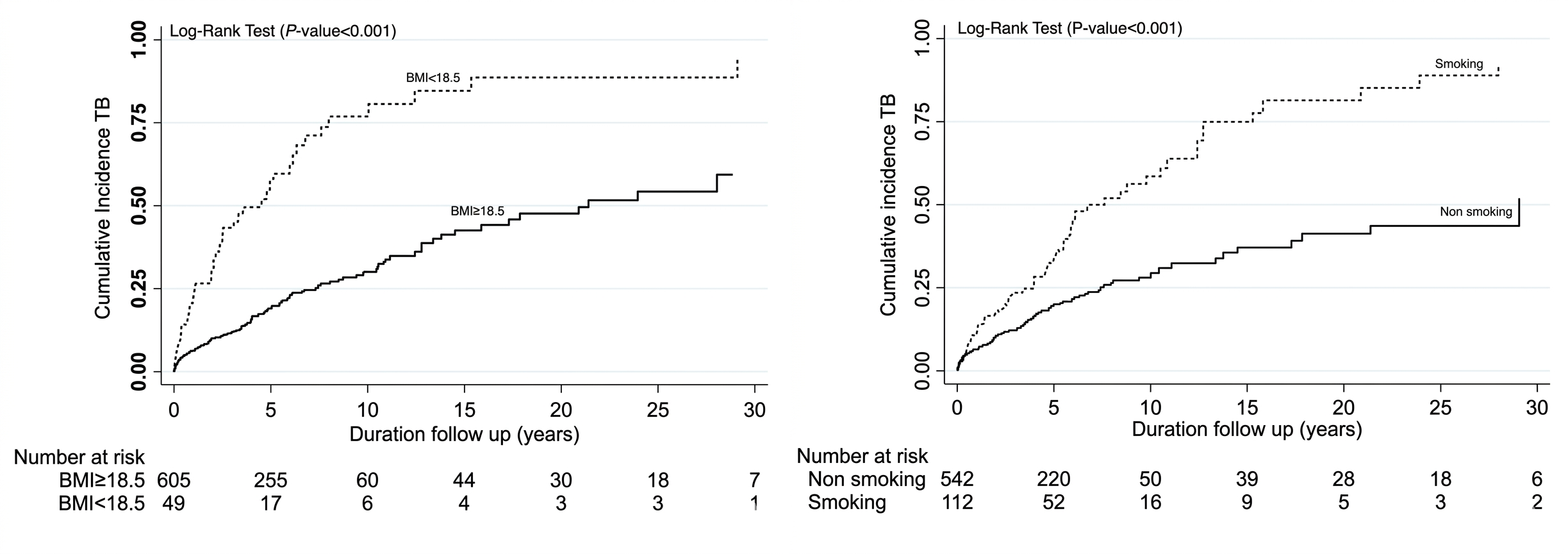
Continuous variables are described using medians and interquartile ranges (IQR), and categorical variables are presented as frequencies and percentages. Chi-square and Kruskal-Wallis were used to formally compare categorical and continuous variables between groups. Kaplan-Meier survival curves and the log-rank tests were used to estimate and compare incidence TB between groups. Cox proportional hazards model was used to determine factors associated with TB.
Ethical consideration
This study was approved by the Institutional Review Board of the Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand (IRB number 262/63); and data collection in the King Chulalongkorn Memorial hospital was authorized by the Information and technology department of the King Chulalongkorn Memorial hospital. The purpose of the research was the study about the risk factors of tuberculosis in patients with diabetes mellitus.
Results
From January 2015 to December 2019, 493 cases of TB in DM patients were recorded in KCMH database. After reviewing the data, 238 of which were excluded from this study, 62 patients were wrong diagnosis, 176 patients had incomplete data record. We included 255 cases of TB in DM patients for the case group. From 37366 cases of DM patients without TB recorded in KCMH database, we randomized by using computer generating command and included 510 cases into the control group. The prevalence of tuberculosis in diabetes patients in KCMH was 1.15% (from January 2015 to December 2019), and 57 (22.3%) first diagnosed diabetic patients at the TB diagnosis. We found that factors that were statistically different between DM with TB and DM without TB were age (>60-year-old), male gender, history of previous smoking, alcohol use, HIV infection, hypertension, dyslipidemia, chronic kidney disease, and treatment of DM (Table 1). But after the Cox proportional hazards model was used to determine the associated factors, we found only the low BMI (<18.5), smoking history and HIV infection were significant (Table 7). Kaplan-Meier found the significant difference of the cumulative TB incidence in diabetes patient between the low BMI and other BMI, smoking and non-smoking (Graph 1). We found the HbA1C at the TB diagnosis was 8 (Table 2).
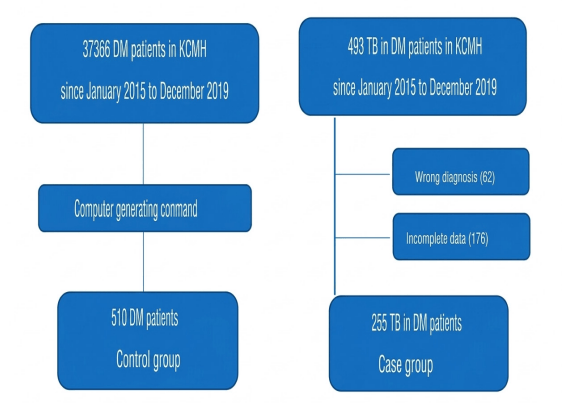
Table 1.Characteristic of patient
| Variables | Total (N=764) |
DM no TB (n=509) |
TB/DM (n=152) |
TB before DM (n=103) |
P-value |
|---|---|---|---|---|---|
| Age, median (IQR) | 62.8 (53.6–72.5) | 63.9 (55.7–73) | 62.1 (52–75.8) | 55.4 (49.4–64.9) | <0.001 |
| Male, n (%) | 407 (53.3) | 231 (45.4) | 116 (64.4) | 60 (80) | <0.001 |
| BMI, median (IQR) | 24 (21.2–26.5) | 25 (22.2–27.4) | 21 (18.8–23.9) | 22 (19.1–24.2) | 0.001 |
| <18.5, n (%) | 63 (8.3) | 10 (2) | 39 (21.8) | 14 (18.7) | <0.001 |
| 18.5–22.9, n (%) | 249 (32.6) | 135 (26.5) | 82 (45.8) | 32 (42.7) | |
| 23–24.9, n (%) | 151 (19.8) | 107 (21) | 30 (16.8) | 14 (18.7) | |
| ≥25, n (%) | 300 (39.3) | 257 (50.5) | 28 (15.6) | 15 (20) | |
| Smoking, n (%) | 152 (19.9) | 55 (10.8) | 61 (33.9) | 36 (48) | <0.001 |
| Alcohol use, n (%) | 163 (21.3) | 71 (14) | 58 (32.2) | 34 (45.3) | <0.001 |
| Underlying, n (%) | |||||
| CVA/TIA | 73 (9.6) | 55 (10.8) | 17 (9.4) | 1 (1.3) | 0.03 |
| HT | 523 (68.5) | 390 (76.6) | 97 (53.9) | 36 (48) | <0.001 |
| DLP | 415 (54.3) | 340 (66.8) | 62 (34.4) | 13 (17.3) | <0.001 |
| TVD | 35 (4.6) | 25 (4.9) | 9 (5) | 1 (1.3) | 0.37 |
| HIV | 18 (2.4) | 4 (0.8) | 11 (6.1) | 3 (4) | <0.001 |
| HBV | 19 (2.5) | 9 (1.8) | 8 (4.4) | 2 (2.7) | 0.14 |
| HCV | 10 (1.3) | 4 (0.8) | 5 (2.8) | 1 (1.3) | 0.13 |
| CKD | 114 (14.9) | 65 (12.8) | 41 (22.8) | 8 (10.7) | 0.003 |
| Complication | |||||
| Yes, n (%) | 231 (30.2) | 157 (30.8) | 60 (33.3) | 14 (18.7) | 0.06 |
| Nephropathy UACR | 123 (53.3) | 82 (52.2) | 32 (53.3) | 9 (64.2) | 0.06 |
| Neuropathy | 5 (2.2) | 4 (2.6) | 0 (0) | 1 (7.1) | |
| Retinopathy | 52 (22.5) | 40 (25.5) | 11 (18.3) | 1 (7.1) | |
| Other (PAD) | 6 (2.6) | 1 (0.6) | 4 (6.7) | 1 (7.1) | |
| ≥2 complications | 45 (19.5) | 30 (19.1) | 13 (21.7) | 2 (14.3) | |
| Treatment DM | <0.001 | ||||
| Oral hypoglycemia | 504 (66) | 380 (74.7) | 82 (50.6) | 42 (82.4) | |
| Insulin injection | 110 (14.4) | 59 (11.6) | 48 (29.6) | 3 (5.9) | |
| Combination | 75 (9.8) | 47 (9.2) | 23 (14.2) | 5 (9.8) | |
| Diet control | 31 (4.1) | 21 (4.1) | 9 (5.6) | 1 (2) | |
| Kidney information | |||||
| Stage | 0.20 | ||||
| •3 | 57 (50) | 30 (46.2) | 21 (51.2) | 6 (75) | |
| •4 | 16 (14) | 13 (20) | 3 (7.3) | 0 (0) | |
| •5 | 41 (36) | 22 (33.9) | 17 (41.5) | 2 (25) | |
| Treatment CKD | 0.11 | ||||
| • Dialysis | 25 (21.9) | 12 (18.5) | 11 (26.8) | 2 (25) | |
| • Kidney transplantation | 8 (7) | 2 (3.1) | 6 (14.6) | 0 (0) | |
| • Medication | 81 (71.1) | 51 (78.5) | 24 (58.5) | 6 (75) | |
| BUN, median (IQR) | 27 (20-45) | 28 (20-44) | 30 (20-47) | 22.5 (20-28) | 0.65 |
| Cr, median (IQR) | 1.9 (1.4-3.7) | 2 (1.5-4.2) | 1.6 (1.3-2.8) | 1.5 (1.4-4.3) | 0.05 |
| eGFR, median (IQR) | 31 (13-47) | 26 (11-43) | 35 (14-50) | 41 (19.5-50) | 0.22 |
Chi-square and Kruskal-Wallis were used to formally compare categorical and continuous variables between groups.
*We observed non-significant in CD4 cell count between group (DM: median (IQR), 316.5 (251-551.5) vs TB+DM: 103 (16-435) vs TB before DM: 474 (16-932); P-value=0.47).
Pulmonary involvement was found in 224 cases (87.8%), and extrapulmonary involvement was found in 31 cases (12.2%), The incidences of culture-confirmed, pulmonary, extrapulmonary, relapsed tuberculosis, the treatment regimen and duration of DM before TB were summarized in table 2. We identified the treatment outcome in table 3, 183 (71.8%) were cured or treatment complete, 5 (2%) were failure of treatment and mortality rate was 12.9%. The incident rate per 1000 person-years follow up was 45.96 (95%CI 39.72-53.19) and total person-time was 3916.18. Drug resistance TB was observed in 37 cases (14.5%) including multidrug resistant TB in 6 cases (2.35%), isoniazid monoresistance in 22 cases (8.63%) and rifampicin monoresistance in 2 cases (0.78%).
Table 2 : Information for TB infection
| Total N=255 | |
|---|---|
| HbA1C at diagnosis, median (IQR) | 8 (6.6–10.3) |
| Types of TB, n (%) | |
| • Pulmonary | 224 (87.8) |
| • Extra-pulmonary | 31 (12.2) |
| Smear: Positive, n (%) | 110 (43.1) |
| Culture TB, n (%) | |
| • Positive | 186 (72.9) |
| • Drug-resistance | 35 (13.7) |
| TB Treatment regimen, n (%) | |
| • 2IRZE+4IR | 161 (63.1) |
| • Other | 94 (36.9) |
| Relapse, n (%) | 17 (6.7) |
| Duration before diagnosis of tuberculosis (years), median (IQR) | 3 (0.7–5.9) |
*HbA1C were new TB (n=180) changes from at diagnosis were assessed with Wilcoxon sign-rank tests. We observed significant decreases in HbA1C (median (IQR) change -0.6 (-2.8 to 0.2) ; P-value<0.001).
Table 3 : Treatment outcome by TB group
| Treatment outcome | Total n (%) | Pulmonary only n (%) | Extra-pulmonary n (%) | P-value |
|---|---|---|---|---|
| Cured or treatment complete | 183 (71.8) | 159 (71) | 24 (77.4) | 0.46 |
| Treatment failed | 5 (2) | 5 (2.2) | 0 (0) | 0.40 |
| Lost to follow up (Culture: Positive at 5th month) |
11 (4.3) | 10 (4.5) | 1 (3.2) | 0.75 |
| Death | 33 (12.9) | 29 (13) | 4 (12.9) | 0.99 |
| Transfer out | 23 (9) | 21 (9.4) | 2 (6.5) | 0.59 |
Table 4 : Incident of drug resistance TB
| Drug resistance | n (%) |
|---|---|
| Multidrug resistance | 6 (2.35) |
| Isoniazid | 22 (8.63) |
| Rifampicin | 2 (0.78) |
| Total | 37 (14.5) |
Table 5 : Incident rate per 1000 person-years follow up
| Total person-time | TB onset (n) | Incident rate | 95% CI | |
|---|---|---|---|---|
| 3916.18 | 180 | 45.96 | 39.72 | 53.19 |
Table 6 : Incident rate per 1000 person-years follow up by Treatment DM
| Treatment DM | Total person-time | TB onset | Incident rate | 95% CI | |
|---|---|---|---|---|---|
| Total | 3827.46 | 162 | 42.33 | 36.29 | 49.37 |
| • Oral hypoglycemia | 2649.79 | 82 | 30.95 | 24.92 | 38.42 |
| • Insulin injection | 613.46 | 48 | 78.24 | 58.96 | 103.83 |
| • Combination | 454.47 | 23 | 50.61 | 33.63 | 76.16 |
| • Diet control | 109.74 | 9 | 82.01 | 42.67 | 157.62 |
Table 7 : Risk factor associated with TB
| Univariate | Multivariate | |||
|---|---|---|---|---|
| HR (95% CI) | P-value | aHR (95% CI) | P-value | |
| Age > 60 | 1.41 (1.05–1.90) | 0.02 | 1.26 (0.89–1.79) | 0.20 |
| Male | 1.78 (1.31–2.42) | <0.001 | 1.08 (0.74–1.60) | 0.68 |
| BMI < 18.5 | 3.73 (2.61–5.33) | <0.001 | 3.78 (2.47–5.78) | <0.001 |
| Smoking | 2.44 (1.79–3.33) | <0.001 | 1.95 (1.23–3.10) | 0.004 |
| Alcohol use | 2.11 (1.54–2.89) | <0.001 | 1.10 (0.66–1.73) | 0.80 |
| Underlying | ||||
| • TVD | 1.05 (0.54–2.06) | 0.88 | ||
| • HIV | 3.14 (1.68–5.87) | <0.001 | 3.31 (1.59–6.86) | 0.001 |
| • HBV | 1.93 (0.95–3.92) | 0.07 | 1.56 (0.69–3.50) | 0.28 |
| • HCV | 2.47 (1.01–6.02) | 0.047 | 1.75 (0.68–4.49) | 0.25 |
| • CKD | 1.58 (1.12–2.25) | 0.01 | 1.52 (0.97–2.37) | 0.07 |
| Complication of DM | ||||
| • No complication of DM | Ref 0.91 (0.65-1.28) | 0.59 | ||
| • One complication of DM | 0.72 (0.40-1.28) | 0.27 | ||
| • Complication of DM ≥ 2 | ||||
| Treatment DM | ||||
| • Oral hypoglycemia | Ref | Ref | ||
| • Insulin injection | 2.58 (1.80–3.70) | <0.001 | 1.60 (1.02–2.51) | 0.04 |
| • Combination | 1.66 (1.04–2.63) | 0.03 | 1.66 (1.02–2.70) | 0.04 |
| • Diet control | 2.36 (1.18–4.71) | 0.02 | 2.50 (1.24–5.04) | 0.01 |
Discussion
The association between diabetes mellitus and tuberculosis has been reported but the previous data are notably scarce, possibly because of the practical difficulty many patients over a prolonged period, and none of the available studies specifically examined diabetic control as reflected by HbA1c. Indeed, notwithstanding the various acute and chronic infections frequently observed among diabetic subjects, relatively little is known about the underlying mechanism(s) or the exact role of diabetic control on infection risks [7,8]. The current study provided the associated factor of the primary impact of diabetic patients on the development of tuberculosis.
In this retrospective study of the risk of tuberculosis among people with DM in KCMH, we found the prevalence of tuberculosis was 1.15%. Compared with the overall prevalence of pulmonary TB in diabetics was shown to be 5.3% [9] which was lower than the estimated prevalence of TB in total population. This finding is in line with the studies conducted in Tanzania (5.4%) [10] and India (6%) [11].
The incident rate per 1000 person-years follow up is 45.96 (95%CI 39.72-53.19) and total person-time is 3916.18 in this study. DM increases the risk of TB by three-fold. (Relative risk 3.11; 95% CI 2.27-4.26) [5,12]. In this study the prevalence is lower than other studies, maybe from the small sample size and the incomplete medical record from the physician. We found 57 (22.3%) first diagnosed diabetic patients at the TB diagnosis, so we suggest for DM screening at TB diagnosis by fasting plasma glucose and hemoglobin A1C.
In this study, we found the average HbA1C of the TB with DM was 8%, it can reflect that the poor glycemic control is the one of associated factors. Because of the poor glycemic control can cause the worse immune status of the diabetes patient, so they are increased risk of tuberculosis. Diabetic mice exhibit a critical delay in adaptive immune priming attributable to defective sentinel function of resident alveolar macrophage [8,13,14]. Once underway, the T cell response in diabetic mice appears to be functionally intact but quantitatively excessive, possibly reflecting higher antigen load and/or defective counter-regulation [8]. Other studies identified that the DM and TB group showed significantly higher levels of HbA1c and postprandial blood sugar, which indicates worse glycemic control compared to diabetics without TB [1,3]. Diabetic control was shown to be the predominant determinant of increased tuberculosis risk. Of some interest is the underlying reason why subjects with well-controlled diabetes mellitus were not at increased risk of pulmonary tuberculosis [4,5].
Low BMI (<18.5) is a significant associated factor in the study. Abera, A. revealed that those DM patients who were underweight (BMI <18.5Kg/m2) had about ten times high odds TB infection with DM. Similar finding was found in a study conducted in Chiayi, Taiwan (15) [OR = 6.635, 95% CI: (2.096-21.007)], a study conducted in India (16) [AOR = 2.03, 95% CI: (1.32– 3.12)] and in Tanzania [17] [OR = 2.08 955 CI: (1.06–4.06)]. BMI indicates malnutrition which is a factor for several infectious diseases. Underweight individuals have a weak immunity system which exposes them to infection [9,8]. But in other studies, showed that being overweight and obesity were risk factors for DM but were protective against TB disease [5,6]. However, weight loss due to poorly controlled DM and metabolic decomposition takes away this protection and becomes risk factor for TB [6].
HIV co-infection is a strongly associated factor in the study. Because of HIV infection people have acquired CMIR defect by immune alteration from the infection, so they can develop active tuberculosis easier than non-HIV patients. HIV status is another important factor strongly associated with TB [2,3].
Smoking history is a significant associated factor in univariate in Cox proportional hazards model in this study but not significant in multivariate method. A study in Taiwan with a cohort of diabetics showed that smoking increases twice the risk of becoming ill with TB. The possible mechanisms that increase a smoker susceptibility to develop TB include a decrease in the immune response due to the dysfunction of ciliary mechanics on the surface of the tracheobronchial mucosa, defects in the immunological response of macrophages, and the reduction of CD4 level [19].
Male gender, older age, alcohol use are tended to be associated factors with developing tuberculosis in diabetes patient but those are not significant. Lifestyle is the important thing that easily leads to infection. Many other studies found that TB-DM comorbidity was significantly more common in patients over 40 years [1]. Because of the worsening of the immune system. Regular drinking is one of the factors that negatively influences adherence to drug treatment, contributing to poor glycemic control and predisposing to complications. In addition, excessive alcohol users are immunologically compromised, which increases the risk of contracting TB as well as the reactivation of latent TB. Although alcohol provides calories, without nutritional support it predisposes to gastric problems, which in turn impair the individual’s nutritional status. Alcohol suppresses monocytes’ ability to produce cytokines, which directly inhibit bacterial growth and play a key role in cell communication, activation, proliferation and migration, as well as regulation of inflammation and healing mechanisms [19].
Regarding TB treatment outcomes, we identified 183 (71.8%) were cured or complete treatment, 5 (2%) were failure of treatment and mortality rate was 12.9%. The mortality rate was too high as compared with other studies that the risk of death from TB or any other causes was nearly 2-fold (RR 1.89; 95% CI 1.52-2.36) [5]. Because of the delayed diagnosis from many causes such as the symptoms aren’t specific or no symptoms, the change in immune system, and improper screening to find out the tuberculosis which causes severe lung destruction.
Multidrug resistant TB was detected in 6 cases (2.35%), Isoniazid resistance TB was 22 cases (8.63%), Rifampicin resistance TB was 2 cases (0.78%). But in other studies, the prevalence of drug-resistant or MDR TB among recurrent TB cases was not significantly higher in TB-DM patients. (OR 1.24, 95% CI 0.72- 2.16) [13].
Conclusion
The incidence of TB among DM cases observed in this study was high and it was associated with low BMI <18.5, smoking and HIV infection, pointing to the need to pay attention to these factors when managing these co-morbidities. Screening TB disease in DM may be another target to achieve better TB control by earlier TB diagnosis and treatment, resulting in reducing TB transmission and better treatment outcomes in TB-DM patients.
References
1. Zheng C, et al. Diabetes and pulmonary tuberculosis: a global overview with special focus on the situation in Asian countries with high TB-DM burden. Glob Health Action. 2017;10(1):1–11.
2. Workneh MH, et al. Prevalence and associated factors of tuberculosis and diabetes mellitus comorbidity: a systematic review. PLoS One. 2017;12(4):e0175925.
3. Hayashi S, Chandramohan D. Risk of active tuberculosis among people with diabetes mellitus: systematic review and meta-analysis. Trop Med Int Health. 2018;23(10):1058–1070.
4. Leung CC, et al. Diabetic control and risk of tuberculosis: a cohort study. Am J Epidemiol. 2008;167(12):1486–1494.
5. Restrepo BI. Diabetes and tuberculosis. Microbiol Spectr. 2016;4(6).
6. Workneh MH, et al. Prevalence and associated factors of tuberculosis and diabetes mellitus comorbidity: a systematic review. PLoS One. 2017;12(4):e0175925.
7. Kumar Nathella P, Babu S. Influence of diabetes mellitus on immunity to human tuberculosis. Immunology. 2017;152(1):13–24.
8. Prada-Medina CA, et al. Systems immunology of diabetes-tuberculosis comorbidity reveals signatures of disease complications. Sci Rep. 2017;7:1999.
9. Abera A, Ameya G. Pulmonary tuberculosis and associated factors among diabetic patients attending Hawassa Adare Hospital, Southern Ethiopia. Open Microbiol J. 2018;12:333–342.
10. Rao P. Persons with type 2 diabetes and co-morbid active tuberculosis should be treated with insulin in Tanzania. Int J Diabetes Dev Ctries. 1999;19:3–5.
11. Lalit K. Diabetes mellitus and tuberculosis: the brewing double trouble. Indian J Tuberc. 2003;50(Suppl 4):1–2.
12. McAllister SM, et al. High tuberculosis incidence among people living with diabetes in Indonesia. Trans R Soc Trop Med Hyg. 2019.
13. Vallerskog T, Martens GW, Kornfeld H. Diabetic mice display a delayed adaptive immune response to Mycobacterium tuberculosis. J Immunol. 2010;184:6275–6282.
14. Martinez N, et al. Impaired recognition of Mycobacterium tuberculosis by alveolar macrophages from diabetic mice. J Infect Dis. 2016;214:1629–1637.
15. Lin YH, et al. Screening for pulmonary tuberculosis in type 2 diabetes elderly: a cross-sectional study in a community hospital. BMC Public Health. 2015;15:3.
16. Viswanathan V, et al. Prevalence of diabetes and pre-diabetes and associated risk factors among tuberculosis patients in India. PLoS One. 2012;7(7):e41367.
17. Faurholt-Jepsen D, et al. The role of anthropometric and other predictors for diabetes among urban Tanzanians with tuberculosis. Int J Tuberc Lung Dis. 2012;16(12):1680–1685.
18. Martinez L, et al. Glycemic control and the prevalence of tuberculosis infection: a population-based observational study. Clin Infect Dis. 2017;65(12):2060–2068.
19. Leal ML, et al. Factors associated with tuberculosis in a population of diabetics: a case-control study. Cien Saude Colet. 2018;24(9):3247–3256.
20. Abedi S, et al. Determinant factors for mortality during treatment among tuberculosis patients: Cox proportional hazards model. Indian J Tuberc. 2019;66(1):39–43.
21. Al-Rifai RH, et al. Association between diabetes mellitus and active tuberculosis: a systematic review and meta-analysis. PLoS One. 2017;12(11):e0187967.
22. Baker MA, et al. The risk of tuberculosis disease among persons with diabetes mellitus: a prospective cohort study. Clin Infect Dis. 2012;54(6):818–825.
23. Nguyen DT, Graviss EA. Diabetic trends and associated mortality in tuberculosis patients in Texas, a large population-based analysis. Tuberculosis (Edinb). 2019;116S:S59–S65.
25. Siddiqui AN, et al. Effect of diabetes mellitus on tuberculosis treatment outcome and adverse reactions in patients receiving DOTS in India: a prospective study. Biomed Res Int. 2016;2016:7273935.
26. Tegegne BS, et al. Association between diabetes mellitus and multi-drug-resistant tuberculosis: evidence from a systematic review and meta-analysis. Syst Rev. 2018;7(1):161.
27. Ugarte-Gil C, et al. Diabetes mellitus among pulmonary tuberculosis patients from four TB-endemic countries: the TANDEM study. Clin Infect Dis. 2019.
28. United Nations. The Sustainable Development Goals Report 2018. 2018.
29. World Health Organization. Global tuberculosis report 2019. 2019.
30. Lin Y, et al. The Union DMTB guide. World Diabetes Foundation. 2018.
Received:February 25, 2026;
Accepted: March 17, 2026;
Published: March 22, 2026.
To cite this article : Choosongdet T, Suwanpimolkul G, Nochaiwong T, Sophonphan J, Avihingsanon A, Kawkitinarong K. Risk Factors of Active Tuberculosis and Tuberculosis Outcomes in Patients with Diabetes Mellitus: A Retrospective Matched Case-Control Study. Eur J Respir Med. 2026; 8(1): 499-505. doi: 10.31488/EJRM.157.
© The Author(s) 2026. This is an open access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/).